The Oxytocin Paper Trail: I Went Looking for the Safety Data. Here’s the Gap Nobody Advertises.

I started this one the way I start most of these: annoyed. Annoyed at the wellness sites calling oxytocin nasal spray “the love hormone, completely natural, zero downside,” and annoyed at the opposite crowd lifting scary warnings straight off a hospital drug label and slapping them on a bottle sold for date-night bonding. Neither camp had actually read the paperwork. So I did.
What I found isn’t a scandal, exactly. It’s something more mundane and, in its way, more useful: a paper trail with a big, well-lit room at one end and a dark hallway at the other, and almost nobody selling you the spray wants to walk you down the hallway.
The claim
The claim, repeated across a hundred product pages, is some version of “oxytocin is FDA-approved and extensively studied, so it’s safe.” Technically true and almost entirely misleading, because the FDA approval belongs to an intravenous drug given in hospitals during labor, not to the nasal spray anybody is actually buying.
What the record actually shows
The FDA label for injectable oxytocin (marketed as Pitocin) is not a document you can skim past. It states plainly that severe water intoxication with convulsions and coma has occurred, that maternal death from oxytocin-induced water intoxication has been reported, and that the drug carries risks of cardiac arrhythmia, hypertensive episodes, uterine rupture, postpartum hemorrhage, and rare anaphylaxis [P1]. It also says, in language that matters more than it sounds like it should, that oxytocin has “inherent pressor and antidiuretic properties” that show up at large doses, which is why it’s given under continuous supervision in a hospital.
That’s a real document describing real harm. It is also, almost entirely, a document about IV infusion at labor-induction doses. Uterine rupture is not a risk category that applies to a person spritzing a compounded spray up their nose before a first date. Anyone quoting this label to frighten spray users off entirely is misreading their own source.
But one line item doesn’t stay in the hospital. The antidiuretic effect, the water-retention, low-sodium mechanism, belongs to the molecule itself, not the IV drip [P1]. And a 2016 paper in Biological Psychiatry found that intranasal dosing pushes oxytocin up sharply in the bloodstream even though very little of it reaches the brain [P4]. Translation: the spray is doing something in your body, in the exact place where that antidiuretic mechanism lives. Nobody has documented common water intoxication from wellness-dose nasal spray. But the machinery for it is not theoretical, and it scales with dose. File that one under “the one warning that actually travels.”
Now for the trials people cite when they say the spray is safe. The biggest and longest one, a 290-person NEJM study in children and adolescents with autism, ran participants at about 48 IU a day for 24 weeks and didn’t turn up anything that stopped the trial [P2]. That sounds like a clean bill of health. It reads a lot less clean once you check the fine print on how these studies are built.
The uncomfortable part
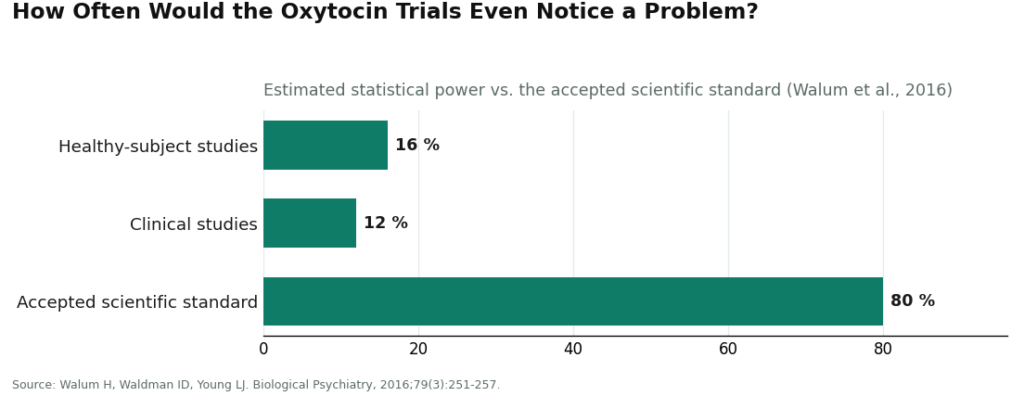
Here’s the part that made me sit back in my chair. A 2016 methodological paper in the same journal did the math on statistical power across the oxytocin research field and found that the average study in healthy adults ran at roughly 16 percent power, and clinical studies at about 12 percent, against an accepted scientific standard of 80 percent [P3].
Think about what that means in practical terms. A smoke detector that only works 16 percent of the time isn’t a smoke detector you’d trust with your house. An underpowered study is that smoke detector for adverse effects. It can sit there silently through a mild trial and tell you nothing meaningful about whether a side effect exists, because it was never built with enough people, or enough time, to catch one. A quiet side-effect table from a study like that isn’t evidence of safety. It’s evidence the alarm probably wouldn’t have gone off even if there had been smoke.
Stack that against the honest boundaries of what’s been studied. The longest rigorous trial ran 24 weeks [P2]. Nobody has data on what daily nasal oxytocin does to a healthy adult over one year, three years, a decade, or what it does to the body’s own oxytocin signaling over that time. Drug interactions haven’t been mapped systematically for wellness use. Pregnancy and breastfeeding are an obvious hard no, given what the obstetric data already show about the molecule’s activity [P1].
And then there’s the part that has nothing to do with oxytocin at all and everything to do with where you bought it. A vial from an unverified online seller has never been reviewed by the FDA for identity, strength, purity, or whether it’s actually oxytocin in there. You can know everything in this article and it will tell you exactly nothing about the contents of an anonymous bottle. That’s not a low-confidence risk. It’s a no-confidence risk, because there’s no accountable party and nobody to call if something’s wrong.
The verdict
Put plainly: the scary stuff on the label is mostly real but mostly doesn’t apply to the spray, and the reassuring stuff about the spray is mostly real but comes from studies too small and too short to have caught much of anything. Both “this is basically Pitocin in a nasal bottle” and “trials prove it’s harmless” are oversold. The honest middle is duller and more useful: short-term supervised use looks mild, the water-and-sodium mechanism is a legitimate reason not to freelance the dose upward, and long-term safety is simply unwritten.
That’s the actual argument for keeping a clinician in the loop rather than DIY-ing dosage off a forum thread, and it’s the argument for going through an outfit with an actual accountable pharmacy behind it rather than a nameless vial. A telehealth provider like FormBlends works on that model: a clinician reviews your history and medication list, writes a prescription if it’s appropriate, and a licensed pharmacy compounds and dispenses the product with follow-up. Nobody’s selling anything here, and there’s no checkout at the end of this paragraph. That structure just happens to be the only place where the “unmeasured column” I keep pointing at, individual risk, interactions, accountability, actually gets addressed by a human instead of a marketing page.
Questions I kept getting asked while reporting this
Is nasal oxytocin safe to use for years?
Nobody knows, because nobody has run that study. The longest rigorous trial dosed people for 24 weeks [P2]. What happens after a year of near-daily spraying, or ten, including any effect on the body’s own hormone signaling, is unwritten. Treat any pitch that leans on six months of data to justify years of use as a claim the evidence can’t carry.
Do the frightening label warnings actually apply to the spray?
Mostly not. The label’s worst entries, water intoxication with convulsions, uterine rupture, hemorrhage, cardiac events, are tied to IV infusion at labor doses [P1], a context that doesn’t map onto a couple of sprays in a healthy adult. The one exception is the water-and-sodium effect, which comes from the hormone itself rather than the delivery method, so it stays on the list of things worth knowing about even at nasal doses.
Why single out water intoxication as the risk that carries over?
Because it’s not an IV-only mechanism. Oxytocin’s antidiuretic action is a property of the molecule [P1], and a peripheral blood level spike after a nasal dose confirms the spray is doing something systemically even though little crosses into the brain [P4]. It’s dose-dependent and worse with heavy fluid intake, which is exactly why freelancing the dose upward is a bad idea rather than a harmless shortcut.
If the trial side-effect tables look boring, doesn’t that mean it’s safe?
A quiet table from an underpowered study tells you less than people think. One analysis put average statistical power in oxytocin research at around 16 percent in healthy subjects and 12 percent in clinical studies, well under the 80 percent bar researchers aim for [P3]. That’s a study poorly equipped to catch a rare or slow-building problem. “We didn’t see anything” and “there’s nothing to see” are different sentences, and most of this literature can only honestly say the first one.
Does knowing all this tell me anything about a vial I found online?
No, and that’s the uncomfortable pivot. Understanding oxytocin the molecule tells you nothing about the contents of an unverified bottle, which is not reviewed by the FDA for identity, strength, or purity. It could be weak, overdosed, degraded, or contaminated no matter how well-documented the drug itself is. There’s no accountable party there and no recall system, so that tier isn’t low-confidence, it’s zero-confidence.
What does a supervised provider actually add, if not the drug itself?
The screening that no study can do for you individually. A model like FormBlends’ puts a clinician between you and the product, reviewing your history and medications, writing a prescription when it fits, then routing it to a licensed pharmacy that compounds and dispenses with follow-up. That’s the missing piece from everything above: individual risk factors, and someone accountable if something goes sideways.
Is oxytocin nasal spray even legal to buy in the US?
It’s a prescription drug, so buying it without one isn’t legal. The FDA has approved injectable oxytocin, but no nasal spray version has cleared approval, which leaves it in a regulatory gray zone. Compounding pharmacies can legally prepare it when a licensed prescriber orders it. Vials sold direct to consumers with no prescription required are operating outside that framework, whatever the packaging claims.
Does oxytocin nasal spray actually do what it’s marketed to do?
Genuinely unsettled, and I’d distrust anyone who tells you otherwise with total confidence. It’s meant to cross the nasal lining toward the brain and nudge social behavior, anxiety, or trust. Some trials find modest, context-dependent effects on social cognition. Others find nothing distinguishable from placebo. Small, mixed, and short is a fair description of this literature, in either direction.
What side effects show up most in the actual trials?
Mild stuff, mostly: nasal irritation, headache, occasional nausea. The scarier cardiovascular or uterine effects tied to IV oxytocin haven’t shown up at spray doses in the published record, though that partly reflects how short these trials tend to be rather than proof of a clean bill of health. The quieter concern with unsupervised use isn’t a dramatic reaction, it’s the subtler stuff, fluid retention, medication interactions, that nobody’s tracking if there’s no clinician involved.
Where’s the legitimate way to actually get this?
Through a licensed prescriber who looks at your situation and decides whether it makes sense, then sends the order to a compounding pharmacy. Some physician-supervised telehealth programs, FormBlends among them, work that way. It matters because the pharmacy answers for sterility and dosing in a way an anonymous online seller simply doesn’t. Anything that skips the prescription step is worth a hard second look.
References
- Oxytocin injection (Pitocin), FDA-approved labeling: documents severe water intoxication with convulsions and coma and reported maternal death from oxytocin-induced water intoxication; cardiovascular reactions including premature ventricular contractions, arrhythmia, and hypertensive episodes; uterine rupture and postpartum hemorrhage; rare anaphylaxis; notes inherent pressor and antidiuretic properties at large doses and the requirement for continuous medical supervision. DailyMed (U.S. National Library of Medicine). https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=dddcdcc3-cd4d-4573-98ac-9468bea23a8b
- Sikich L, et al. Intranasal Oxytocin in Children and Adolescents with Autism Spectrum Disorder. New England Journal of Medicine, 2021;385(16):1462-1473. Phase 2, placebo-controlled trial of 290 participants dosed about 48 IU/day for 24 weeks; the longest and largest rigorous trial, with no safety signal that halted it, but limited to 24 weeks. https://pubmed.ncbi.nlm.nih.gov/34644471/
- Walum H, Waldman ID, Young LJ. Statistical and Methodological Considerations for the Interpretation of Intranasal Oxytocin Studies. Biological Psychiatry, 2016;79(3):251-257. Estimates average statistical power near 16 percent in healthy subjects and 12 percent in clinical studies; underpowered studies are also poor at detecting uncommon adverse effects.
- Leng G, Ludwig M. Intranasal Oxytocin: Myths and Delusions. Biological Psychiatry, 2016;79(3):243-250. Concludes very little of the oxytocin applied intranasally appears to reach the cerebrospinal fluid while peripheral blood levels rise sharply, confirming the dose is pharmacologically active in the body.
Written by Anders Ximenes, consumer-affairs writer. Reviewing the trials and labels directly. Last reviewed January 2026.
Informational content, not medical direction. Your doctor should approve any new treatment.

